This is part of a series on the Novel Coronavirus (COVID-19) pandemic.
There are many factors intervening in a society’s ability to combat disease. While Italy was featured everywhere in global media as the place where COVID-19 was out of control and the situation desperately stark, the spreading of the virus was showing more and more its uneven impact.
In terms of infected individuals and casualties, the early impact of COVID-19 in Italy was more severe in the North than the South. Because the data is incomplete, it may be still too early to draw accurate and final conclusions on COVID-19, however, experts in the field have put forth some explanations for this unevenness.
According to Varrella (2020), as per July 3, 2020, there were 10,891,872 cases of COVID-19 in the world. In Italy, 240,436 cases were registered on June 29. On that date, the regional distribution data showed that, in the northern regions, 93,839 cases were recorded in Lombardy, 31,338 cases in Piedmont, and 28,472 in Emilia Romagna. In the southern regions, which include the Southern peninsula, Sardinia, and Sicily, 4,666 cases were registered in Campania, 3,068 in Sicily, and 1,180 in Calabria.
Possible causes for the North-South discrepancy
Several explanations have been offered by experts on why the South suffered fewer casualties than the North. First, news of the outbreak of COVID-19 in the North of Italy gave the authorities in the South time to prepare and impose drastic restrictions that were observed by their citizens. Other arguments are demographic and economic. In 2019, the total Italian population was 27 million—8 million in the North, 12 million in the Center, and 20.5 million in the South (Tuttitalia.it 2020). Northern Italy features high population density and its productive and economic fabric consists of many companies and businesses of small to large size distributed on its territory and located close to each other. This fabric requires incessant professional and working contacts and high mobility through commuting via an efficient public transportation system (bus, subway, and train). The higher standard of living in the North compared to the South also supports numerous services such as bars, restaurants, clubs, and other places of entertainments (stadiums, museums, parks, etc.) that were not immediately closed and thus favored contagion. Paradoxically, the high number of hospitals in the North might have spread the virus, at least initially, in the face of inadequate precautions and restrictions. In the South, some COVID-19 cases may actually have been due to infected family members fleeing from the North to the South (Zorzut 2020).
In March, in the early stage of the pandemic, Dr. Guido Silvestri, Professor of Pathology and Laboratory Medicine at Emory University (Atlanta, GA) as well as other observers, proposed the following reasons for the high numbers of recorded COVID-19 cases and deaths in Northern Italy (Laganà, 2020):
- Presence of pre-existing infections not diagnosed earlier
- Erroneous attribution of deaths to COVID-19, i.e. death “with” COVID-19 but not “due to” it
- Lower temperature and higher humidity compared to the South
- Environmental pollution
- Higher average age of the population compared to the South. In fact, in 2019, the percentage of residents aged over 65 was 23.9 percent in the North and only 21.6 percent in the South (Carrino 2020).
- Social contact between seniors and youngsters
- High number of hospitalized patients in a short period of time
- A genetic and more aggressive mutation of COVID-19.
Observers have argued that Southern authorities acted faster than Northern authorities and imposed more severe restrictions than the North, thus reducing the number of patients and casualties there (Dente 2020). However, Horowitz et al. (2020) pointed out that Giacomo Grasselli, coordinator of intensive care units throughout Lombardy, when seeing the dramatic increase in the number of infections, realized that the regional health system was facing a catastrophic situation. The President of Lombardy Attilio Fontana, who had already asked the central government to take tougher action, agreed with Grasselli, saying that the conflicting messages from the central government in Rome had led Italians to believe “that it was all a joke, prompting them to continue living as before.” Fontana reiterated his call for more restrictive measures at the national level during videoconferences with the Prime Minister and other regional presidents, arguing that a growing number of cases would put the hospital system in the North at risk of collapse, but his requests were repeatedly rejected. “They were convinced that the situation was less serious and did not want to damage our economy too much,” said Fontana.
In April, Giovanni Rezza, head of the Department of Infectious Diseases of the Public Health Institute (part of the National Health Service), confirmed that the effectiveness of the response in the South had been facilitated by having time to prepare against COVID-19 (Florio 2020). This conclusion seems to be backed by Doctor Roberto Cauda (2020), professor of infectious diseases at the University Hospital Policlinico Gemelli in Rome. According to him, not only imposing lockdown in April, before COVID-19 reached the South, surely helped contain the number of infected and deceased people there, but warm temperatures were possibly also a mitigating factor.
The effective and skilled response by sanitary structures in the South also contributed to contain the spread of COVID-19. In fact, on March 31, the British broadcaster and telecommunications company Sky UK aired a video recorded inside Cotugno Hospital in Naples, praising it as a model in treating COVID-19 patients and the only Italian hospital without casualties among its doctors and nurses. At Cotugno, doctors and nurses leveraged their long experience in dealing with infectious diseases like cholera, HIV, SARS, and Ebola (Viola 2020). They followed very strict and pervasive measures to contain the spread of the virus, and utilized advanced protective equipment.
Air pollution, temperatures, and intergenerational contacts
Mario Coccia (2020), Research Director at National Research Council of Italy with appointments at Yale and Arizona State University, published a study on the factors determining the diffusion of COVID-19 in Italy based on data on its infected inhabitants as of April 7. He observed that the transmission dynamics of COVID-19 were due to two mechanisms: transmission among people and transmission from air pollution to people (airborne viral infectivity). The latter phenomenon might have been stronger than the former. Coccia analyzed data from the Italian Ministry of Health relative to a sample of fifty-five Italian province capitals, and his analysis indicated that the rapid and vast diffusion of COVID-19 in Northern Italy was strongly associated with air pollution of cities measured in days exceeding the limits set for PM10 (particulate matter 10 μm or less in diameter) and ozone. He pointed out that: a) a very large number of infected individuals was recorded in towns with more than one hundred days of air pollution, and b) in inland polluting towns featuring slow winds, diffusion of viral infectivity accelerated, and infected individuals were more numerous than in coastal towns. Coccia’s conclusion about pollution seems confirmed by Figure 1, a satellite image of Southern Europe and Italy that was taken by European Space Agency (ESA), which displays the concentration of nitrogen dioxide NO2 (an indicator of air pollution) in values ranging from yellow (lower concentration) to red (higher concentration). The upper and lower images were taken respectively before (January 2020) and after (February-March 2020) the quarantine and lockdown. Lombardy and Milan are indicated by the white arrow, and located at the edge of the most polluted area in Italy, coinciding with the river Po valley. Coccia also mentioned that sunny and hot weather resulting in lower air pollution and higher production of vitamin D in people reinforces and improves the ability of immune systems to cope with COVID-19 and other diseases. Therefore, we could speculate that if relatively warm weather occurred in the South of Italy during the period of time analyzed by Coccia (as it is reasonable to expect), that might have contributed to slowing down the diffusion of COVID-19 in the South, among other factors.
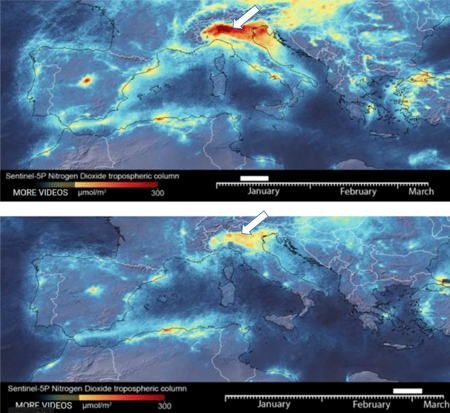
Figure 1: Satellite map of Southern Europe and Italy displaying the concentration of nitrogen dioxide NO2 across Italy before (upper image) and after (lower image) the quarantine and lockdown. White arrows point to Lombardy, and Milan.
A team of Italian researchers explored the possibility that extensive intergenerational contact was a cause of the severity of the pandemic among the Italian older adults (Liotta et al. 2020). They tested this hypothesis by analyzing other variables, such as the percentage of infected patients over eighty, available nursing home beds, COVID-19 incidence rate, number of days until the number of positive tests exceeded fifty cases at regional level (epidemic maturity), mean household size, and percentage of single-person households within the region. The pandemic was more severe in regions with higher family fragmentation and increased availability of residential health facilities. The latter factor seems to be confirmed, according to us, by the fact that the 2001 census reported that the number of seniors living in residential health facilities per 10,000 inhabitants was seventy-nine in the North and twenty-three in the South (ANLA n.d.). The pairing of social connectedness with the spread of COVID-19 among Italian older adults was not confirmed. Paradoxically, it seemed that social isolation was a risk factor for increasing the cases in Italian patients older than eighty This is consistent with the observation that social relationships are a protective factor against increased mortality rates during a crisis impacting the frailest groups of population.
Mismanagement and communication strategies
In her article Mismanagement of Covid-19: lessons learned from Italy (2020), Ruiu analyzes the political, media, and scientific responses to the COVID-19 outbreak in Italy and the critical aspects of their combined efforts (Glik 2007). Citing Houston et al. (2015), she stresses that “communication strategies are an essential component of disaster planning, response, and recovery” (Ruiu 2020: 2). Building trust is one the main goal of such a strategy (Covello et al. 2001; Glik 2007), and the capacity of reaching this goal can determine the success of a response to a critical situation. The agreement between scientists and decision-makers is one of the pillars on which trust is built, while its absence can affect people’s reaction to a crisis (Brug et al. 2004; Eriksson 2018). Talking about the role of communication and miscommunication, Ruiu reminded that “some panic reactions increased the exposure of the South of the country to the virus. The content of the government plan to lockdown the Lombardy region leaked on the 7th of March” (Ruiu 2020, 7). This critical factor prompted a massive attempt to flee to the South of Italy and forced the Southern regions to implement even more restrictive measures. Communication in Italy failed in several ways. First, there were mixed messages from multiple sources, which were worsened by the lack of coordination between scientific and governmental messengers. Secondly, there was a delay in releasing information, as well as chaotic and competing media communication. A coordinated communication process in a univocal direction and political and scientific cohesion should have been applied (Ruiu 2020).
Local community response in the South
In this time of restrictions imposed to prevent the spread of the pandemic, solidarity in the territories is increasing, reshaping local actions, mobilization and fostering self-organized initiatives in support of those in need. (Cattivelli and Rusciano 2020, 2).
Initiatives proliferated in Naples province for example, which has been one of the most affected in the South by the spread of COVID-19. The support to citizens in difficulty included the implementation of food security measures, such as food banks, canteens, and other projects (Signori and Forno, 2019). One of these initiatives recovered the ancient Neapolitan custom of leaving an already-paid-for coffee at the local cafe for the people in need: the caffè sospeso, which means suspended coffee. The current version of this initiative aims at reaching a much wider population than the customers at local cafés. It includes the donation of food, medicines, and other basic necessities to those who are in a state of need by leaving products at the store checkout. The donations are “reported with a WhatsApp message or a phone call at the same time as a fundraiser has been activated. The first institution to activate this form of solidarity spending in Naples is the Municipality” (Cattivelli and Rusciano 2020, 8). The role of the network created among local agencies and businesses and voluntary associations is important, as is that of social media, such as Skype and YouTube (Cattivelli and Rusciano, 2020; Tracey and Stott, 2016).
Medical schools in the South of Italy: The past and the present
Physicians and nurses’ response has contributed to the containment of COVID-19 casualties in the South of Italy. This response stems from a long-standing practice in the study of medicine in the region, which is traceable back to the fifth century B.C., and has continued over time until today with specialists who have excelled at national and international levels. Archeological finds in Velia (140 km south of Naples) dating to about fifth century B. C., namely busts of healers and physicians and inscriptions mentioning them (Mastronuzzi 2015; Udai 2012) testify to a very long tradition of medical expertise in Southern Italy, dating back to at least twenty-five centuries ago. The Scuola Salernitana, which was founded in the ninth century out of the dispensary of a monastery, was the first and most important medical schools in Europe at the time, and even accepted women as professors and students (De Renzi 2002; Greco 2020; Jaquart et al 2008; Nigro 2004).
When the University of Naples (the oldest public non-sectarian university in the world) was founded in 1224, it included a school of medicine (Scuola di Medicina e Chirurgia di Napoli. n.d.). From the eighteenth century on, Southern Italy led the rest of Italy in terms of public healthcare assistance and structures. Today, physicians and hospitals in Southern Italy operate at levels of national and international excellence, for example implanting the world’s smallest pacemaker (La Sicilia 2019), carrying out the world’s first two mini-invasive operations of robotic surgery (Hybrid Robotic Video Assisted Thoracoscopy Surgery) at the thorax (NapoliToday 2019), and continuing to produce scientists of world prominence, like geneticist Andrea Ballabio. This longstanding tradition created the basis for the excellence that brought Stuart Ramsay (2020), Sky News correspondent, to visit the Cotugno Hospital in Naples and comment that the procedures in place there to protect personnel and treat patients were at a level “never seen before,” pointing out that not a single member of Cotugno’s medical teams had been affected. Therefore, Ramsay noted, the fact that many health workers and patients had succumbed to COVID-19 in the North perhaps was not inevitable. And certainly, it was not inevitable at the Cotugno Hospital.
North-South discrepancies: many interconnected factors
In retrospect, it appears that the North of Italy was more severely impacted by COVID-19 because of its high levels of air pollution, high population density and mobility, delay in imposing restrictions, the spreading of the virus among patients and visitors in hospitals that were not prepared for dealing with this infectious disease, family fragmentation, and increased availability of residential health facilities. The South, on the other hand, benefited from immediate and early implementation of strict and general restrictions, warm temperatures and low humidity, time to prepare against the virus, and possibly fewer seniors living in residential health facilities. It also benefited from the presence of hospitals like the Cotugno in Naples, which not only managed to effectively treat COVID-19, but also to save the lives of the precious personnel treating and supporting the patients, as to become an example of excellence in Italy and abroad.
The current crisis prompted by COVID-19 also shed some light on the issues that the countries that are dealing with this infectious disease might want to address. With reference to Italy, Indolfi and Spaccarotella (2020) reminded that “social containment, early and rapid throughout a nation, is the most effective measure for controlling the spread of COVID-19” (2020, 1414). In their insightful analysis, they concluded that:
This catastrophe will be very helpful for Italy and other countries in terms of rethinking the health organization of the future and rebuilding an even more efficient health system. The lesson that Italy has learned from this pandemic is that we must be prepared, and we must always plan for the worst and hope for the best scenario. Italian politicians should rethink the linear cuts made in recent years to public health, as well as to the reduction in the number of doctors, residents, beds, and resources to maintain the quality of medical services in all Italian regions (2020, 1417).
This is certainly what we also hope for Italy and for all the countries that are affected by COVID-19 and the impact of the unprecedented challenges that millions of people are facing all around the world.
Angela Cacciarru is a political ecologist trained in the fields of human geography, urban and regional planning, and development studies, with research interests in land tenure’s role on development patterns, in resource access and exploitation, with particular focus on food security, sustainable food production, and water management. She developed her international and interdisciplinary background in the United States, Europe, and Southern Africa, and got her Ph.D. in Human Geography at the University of North Carolina at Chapel Hill.
Antonio Paesano holds a Ph.D. in mechanical engineering from University of Naples (Italy). He works at Boeing as technical lead in R&D applied to engineering materials, manufacturing processes, testing and analysis, data analysis, and additive manufacturing. In these areas, he holds six patents, authored two book chapters, and authored and coauthored fifty technical papers.
References:
ANLA n.d. “Guida alle Strutture Residenziali per Anziani in Italia, p. 4.” http://www.anla.it/documenti/pdf/progettocdr.pdf.
Brug, Johannes, Arja R Aro, Anke Oenema, Onno de Zwart, Jan Hendrik Richardus, and George D Bishop. 2004. “SARS Risk Perception, Knowledge, Precautions, and Information Sources, The Netherlands.” Emerging Infectious Diseases 10 (8): (August 2004): 1486–1489. doi:10.3201/eid1008.040283.
Carrino Antonella, 2020. “Indicatori Istat 2019: l’età media sale ancora. Siamo a 45,7 anni”. Spazio50. February 12.https://www.spazio50.org/indicatori-istat-2019-leta-media-sale-ancora-siamo-a-457-anni/.
Cattivelli, Valentina, and Vincenzo Rusciano. 2020. “Case Report Social Innovation and Food Provisioning during Covid-19: The Case of Urban–Rural Initiatives in the Province of Naples” Sustainability 12 (11): 4444. doi:10.3390/su12114444.
Cauda, Roberto. 2020. “Al Nord 10 Volte I Casi Della Campania/ Perché il coronavirus ha risparmiato il sud?” ilSussidiario.net. April 27. https://www.ilsussidiario.net/news/al-nord-10-volte-i-casi-della-campania-perche-il-coronavirus-ha-risparmiato-il-sud/2012814/.
Coccia Mario. 2020. Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Science of the Total Environment 729:138474. doi: 10.1016/j.scitotenv.2020.138474.
Covello, Vincent T., Richard G. Peters, Joseph G. Wojtecki, and Richard C. Hyde. 2001. “Risk Communication, the West Nile Virus Epidemic: responding to the Communication Challenges Posed by the Intentional and Unintentional Release of a Pathogen in an Urban Setting.” Journal of Urban Health: Bulletin of the New York Academy of Medicine 78 (2): 382–391. doi:10.1093/jurban/2.382.
De Renzi, Salvatore. 2002. Storia documentata della Scuola medica salernitana (rist. anast. 1857). Napoli: Tip. di Gaetano Nobile.
Dente, Emanuela. 2020. “Come mai il coronavirus ha avuto un impatto piu’ lieve nel Sud Italia? La risposta degli scienzati.” L’Occhio. April 11. https://www.occhionotizie.it/meno-casi-coronavirus-sud-italia-ragioni/.
Eriksson, Mats. 2018. “Lessons for Crisis Communication on Social Media: A Systematic Review of What Research Tells the Practice.” International Journal of Strategic Communication 12 (5): 526-551. doi: 10.1080/1553118X.2018.1510405.
Florio, Felice. 2020. “Coronavirus, come mai al Sud non è esplosa l’emergenza? Rezza: «Il fattore temporale ha salvato il Meridione» L’intervista.” Open. April 12. https://www.open.online/2020/04/12/coronavirus-come-mai-al-sud-non-e-esplosa-emergenza-rezza-il-fattore-temporale-ha-salvato-il-meridione-intervista/.
Glik, Deborah C. 2007. “Risk Communication for Public Health Emergencies.” Annual Review of Public Health 28 (1): 33–54. doi: 10.1146/annurev.publhealth.28.021406.144123.
Greco, Pietro. 2020. Trotula. La Prima Donna Medico d’Europa. Roma: L’Asino d’Oro Edizioni.
Houston, J. Brian, Joshua Hawthorne, Mildred F Perreault, Eun Hae Park, Marlo Goldstein Hode, Michael R Halliwell, Sarah E Turner McGowen, Rachel Davis, Shivani Vaid, Jonathan A McElderry, and Stanford A Griffith. 2015. “Social Media and Disasters: A Functional Framework for Social Media Use in Disaster Planning, Response, and Research.” Disasters 39 (1): 1–22. doi:10.1111/disa.12092.
Indolfi, Ciro and Spaccarotella, Carmen. 2020. “The Outbreak of COVID-19 in Italy. Fighting the Pandemic” JACC. Case Reports, no 9 (2): 1414-1418. https://casereports.onlinejacc.org/content/2/9/1414. doi: https://doi.org/10.1016/j.jaccas.2020.03.012.
Jacquart, Danielle, and Agostino Paravicini-Bagliani, eds. 2008. La «Collectio salernitana» di Salvatore De Renzi. Florence: Edizioni del Galuzzo.
La Sicilia. 2019. “Nell’ospedale di Taormina impiantato il pacemaker più piccolo al mondo.” LaSicilia. July 5. https://www.lasicilia.it/news/messina/172975/nell-ospedale-di-taormina-impiantato-il-pacemaker-piu-piccolo-al-mondo.html.
Laganà, Gabriele. 2020. “Tutti i possibili motivi dell’alto numero di decessi nel Nord Italia.” ilGiornale.it, March 22. https://www.ilgiornale.it/news/cronache/coronavirus-silvestri-ecco-i-possibili-motivi-dell-alto-1844481.html.
Liotta, Giuseppe, Maria Cristina Marazzi, Stefano Orlando, and Leonardo Palombi. 2020. “Is social connectedness a risk factor for the spreading of COVID-19 among older adults? The Italian paradox.” PLoS ONE (5):e0233329. https://doi.org/10.1371/journal.pone.0233329.
Mastronuzzi, Giovanni. 2015. “Immagini di poeti e filosofi della Magna Grecia.” In Cinque incontri sulla Cultura Classica, edited by Mario Capasso, 55-69. Lecce: Pensa Multimedia. https://www.academia.edu/17647406/Immagini_di_poeti_e_filosofi_della_Magna_Grecia_in-Cinque_incontri_sulla_cultura_classica_a_cura_di_M._Capasso.
Napolytoday. 2019. “Ospedale Monaldi, eseguiti due interventi straordinari con chirurgia robotica.” Napolytoday, January 20. https://www.napolitoday.it/salute/interventi-chirurgia-robotica-monaldi-napoli.html.
Nigro, Paola. 2004. La Scuola Medica Salernitana, Giffoni Valle Piana (SA): Ripostes.
Ramsay, Stuart. 2020. Coronavirus: The Italian COVID-19 hospital where no medics have been infected. Sky News, March 31. https://www.youtube.com/watch?v=RsJJtI9bwwo.
Ruiu, Maria Laura. 2020. “Mismanagement of Covid-19: lessons learned from Italy” Journal of Risk Research. https://doi.org/10.1080/13669877.2020.1758755.
Scuola di Medicina e Chirurgia di Napoli. n.d. Università degli Studi della Campania. La Storia. http://www.medicina.unina2.it/it/la-scuola/sedi-della-facolta/la-storia.
Signori, Silvana, and Francesca Forno. 2019. “Consumer groups as grassroots social innovation niches” British Food Journal 121 (3): 803–814.
Tracey, Paul, and Neil Stott. 2016. “Social innovation: A window on alternative ways of organizing and innovating” Innovation 19 (1): 51–60. doi: 10.17863/CAM.7990.
Tuttitalia.it. 2020. “Statistiche Demografiche. Nord, Centro e Mezzogiorno d’Italia.” Accessed August 28. tuttitalia.it. https://www.tuttitalia.it/statistiche/nord-centro-mezzogiorno-italia/.
Udai, Nath B. 2012. “Parmenide filosofo e guaritore sacro. Il viaggio ultraterreno dello iatromante e l’origine sciamanica della filosofia” Visionaire Blog, October 1. https://blog.visionaire.org/2012/10/parmenide-filosofo-e-guaritore-sacro/.
Varrella, Simona. 2020. “Coronavirus (COVID-19) in Italy – Statistics & Facts.” Statista, August 14. https://www.statista.com/topics/6061/coronavirus-covid-19-in-italy/.
Viola, Vera. 2020. “Coronavirus, il Cotugno di Napoli è l’ospedale modello con zero contagi.” Il Sole 24ore, April 2. https://www.ilsole24ore.com/art/coronavirus-cotugno-napoli-e-l-ospedale-modello-zero-contagi-ADIkSjH.
Zorzut, Fulvio. 2020. “Perché l’epidemia non ha sfondato al Sud? Un’opinione medica.” Trieste All News, July 5. https://www.triesteallnews.it/2020/05/07/perche-lepidemia-non-ha-sfondato-al-sud-unopinione-medica/.
Figure 1 Source: European Space Agency (ESA). Copyright by ESA. Contains modified Copernicus Sentinel data (2020), processed by ESA, CC BY-SA 3.0 IGO. Reproduced with permission.
Photo: MILAN, ITALY-MARCH 15, 2020: the empty Duomo square due to the coronavirus’s emergency, in Milan | Shutterstock
Published on September 8, 2020.